
美國腸胃科醫學會(AGA)最新臨床指引:依據不同 HBV 再活化風險的預防與治療建議
Adapted from Ali FS, et al. Gastroenterology. 2025;168:267-284.
精華要點
- 不同類別的藥物與疾病狀態均有可能引起 HBV 再活化(HBVr),預防性使用抗病毒藥物則可有效降低風險。
- AGA 最新發表的 HBVr 預防與治療指引,根據 HBVr 風險的不同,分別提出預防與治療建議。
- 不同類別的藥物與疾病狀態均有可能引起 HBVr,HBVr 的發生率會隨著免疫抑制的程度和機制而有所差異,其中 B cell-depleting agents(例如 rituximab)是常見具有 HBVr 高度風險的藥物。而預防性使用抗病毒藥物(antiviral prophylaxis),則可有效降低 HBVr 的發生風險。
- 針對有 HBVr 風險的病人,美國腸胃科醫學會(AGA)於 2025 年發表了最新預防與治療臨床指引,有助於臨床醫師擬定藥物治療策略。
AGA 之 HBVr 風險評估與處置建議
- AGA 指引建議,對於具有風險的個案應進行 HBVr 評估,建立起病人的基線期血清學資料,建議的檢查項目包括 HBsAg、anti-HBc 和 HBV DNA。
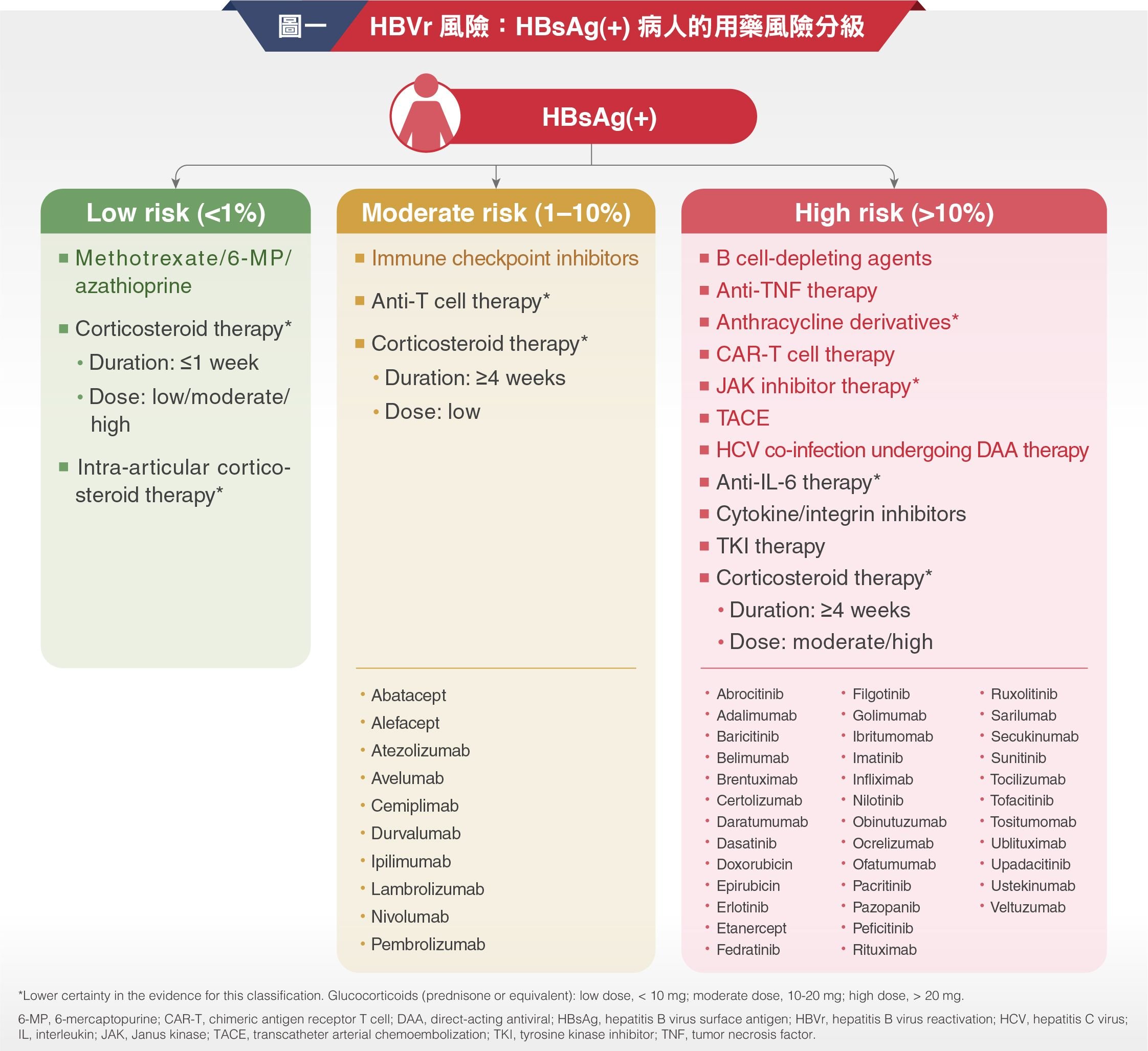
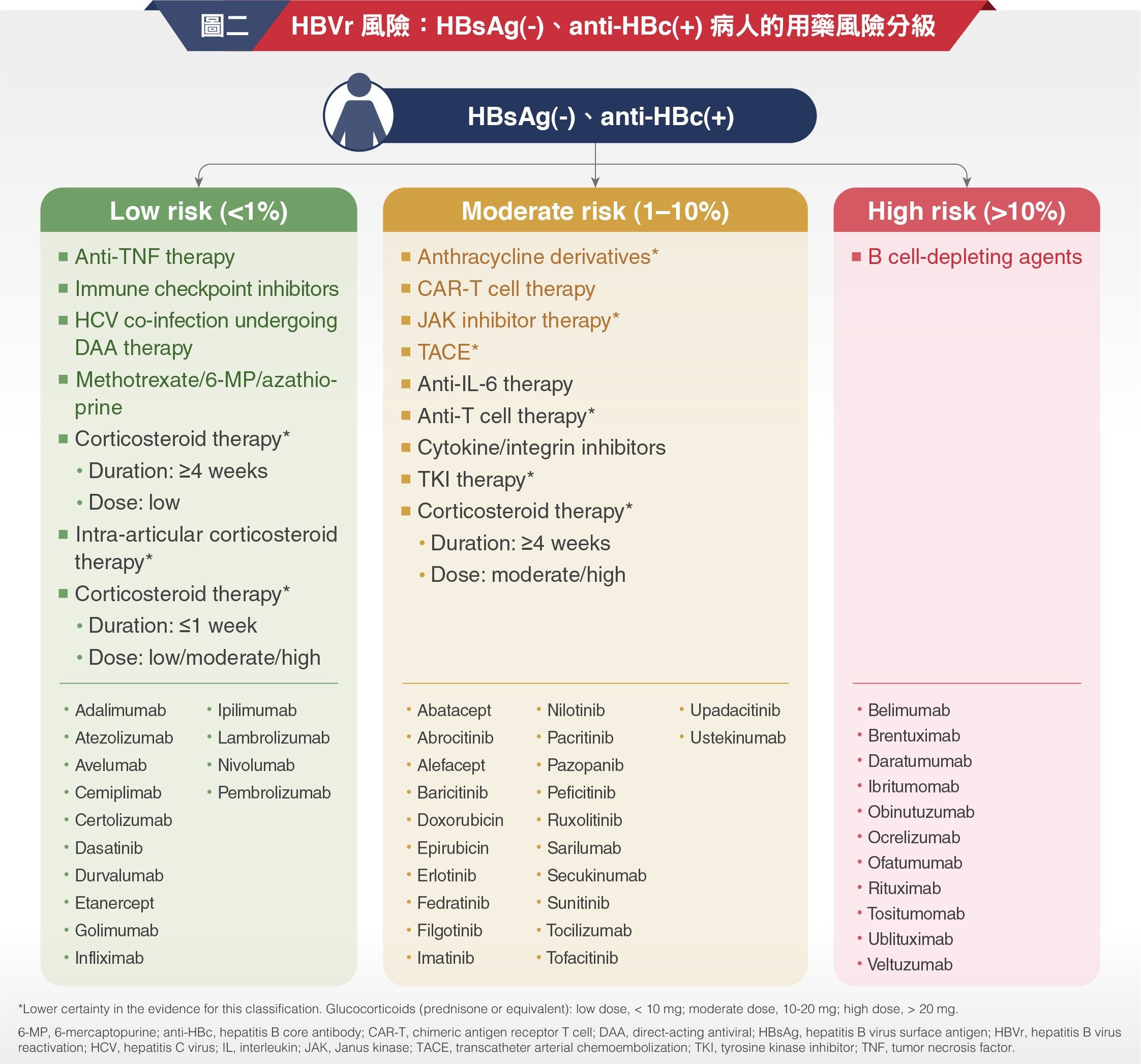
- HBsAg(+) 病人和 HBsAg(-)/anti-HBc(+) 病人的用藥風險分級摘要分別如圖一與圖二。針對 HBVr 高風險和中風險族群,AGA 均建議優先使用抗病毒藥物進行預防性治療,而非僅進行監測(分別為強烈建議和有條件建議、均為中度確定性證據)。至於低風險族群,AGA 則建議優先進行監測,而非預防性使用抗病毒藥物(有條件建議、中度確定性證據) 。
AGA 之 HBVr 預防與監測建議
- 對於具有高度 HBVr 風險的病人,在開始使用可能引起 HBVr 的藥物治療前,應先行給予預防性抗病毒藥物,並且在高風險藥物停用之後,抗病毒藥物治療仍應持續至少 6 個月。
- 對於具有中度 HBVr 發生風險的病人,應先行給予預防性抗病毒藥物。若患者選擇不使用藥物預防,則建議每 1-3 個月進行監測,監測項目必須包含 HBV DNA。
- 無論是高度或中度 HBVr 風險族群,在給予預防性抗病毒治療時,均建議使用高抗藥性屏障的藥物。
- 因 B cell-depleting agents 可能導致延遲性 HBVr 的發生,因此預防性抗病毒治療應延長至 B cell-depleting agents 停藥後至少 12 個月。
- 有鑑於美國疾管局已建議所有 ≥ 18 歲的成人應進行 HBV 篩檢,篩檢項目包括 HBsAg、anti-HBs 和總 anti-HBc,因此不需要再依 HBVr 風險的大小進行分層篩檢。
結語
- AGA 發表的最新 HBVr 預防與治療指引,根據現有研究證據與病人的基線期風險評估結果,提出下列 4 項建議:
- 高風險病人:強烈建議預防性使用抗病毒治療。
- 中風險病人:有條件建議預防性使用抗病毒治療。
- 低風險病人:有條件建議僅需進行監測,而非預防性使用抗病毒治療。
- 對於具有 HBVr 風險的個案:強烈建議進行 HBV 檢測,檢測項目包括 HBsAg、anti-HBs 以及總 anti-HBc。
Abbreviations: 6-MP, 6-mercaptopurine; AGA, American Gastroenterology Association; anti-HBc, hepatitis B core antibody; anti-HBs, hepatitis B surface antibody; CAR-T, chimeric antigen receptor T cell; DAA, direct-acting antiviral; DNA, deoxyribonucleic acid; HBsAg, hepatitis B virus surface antigen; HBV, hepatitis B virus; HBVr, hepatitis B virus reactivation; HCV, hepatitis C virus; IL, interleukin; JAK, Janus kinase; TACE, transcatheter arterial chemoembolization; TKI, tyrosine kinase inhibitor; TNF, tumor necrosis factor.
Reference: Ali FS, et al. AGA clinical practice guideline on the prevention and treatment of hepatitis B virus reactivation in at-risk individuals. Gastroenterology. 2025;168:267-284.
